









Cardiovascular disease (CVD) is the leading cause of mortality globally. It is estimated that around 17.9 million people died from CVD in 2019, so it accounted for nearly 32% of all global deaths.1,2 The prevalence of CVD is expected to rise in the future because of rising obesity and increasingly unhealthy lifestyles as well as an ageing population.3 The majority of deaths from CVD occur in low- and middle-income countries, including those in the Asia-Pacific region.1,2 There is an urgent need to identify methods to improve the outcomes of those with CVD.
In many individuals with CVD, one of the most dangerous clinical manifestations is acute coronary syndrome (ACS), particularly ST-elevation MI (STEMI) and non-STEMI, which carries a significant mortality risk.4 While many international and national guidelines have been published to assist healthcare professionals in providing the best recommended treatment strategies, the majority of patients presenting with ACS often do not receive this.4–6
Registries are an important tool for collecting information from large datasets that can be used to inform decision-making.7 They act as a tool for local quality control, audits and benchmarking against treatment aims and outcomes. Information obtained from them can be used to determine the appropriateness of care according to local/international clinical practice guidelines and the effectiveness of care for individuals with CVD. This information can provide new insights into patient demographics and clinical characteristics as well as a real-world view of clinical care that can be used for scientific, clinical or policy purposes.
Several global ACS and CVD registries have been established, such as the Myocardial Ischaemia National Audit Project (MINAP) and the Global Registry of Acute Coronary Events (GRACE), but only a few countries have established their own national CVD or ACS registries. This gap has been well recognised, and several countries have set up some form of ACS registry. A recent study demonstrated there had been increase in ACS registries over the past decade, with most of them in Europe.6 Nevertheless, despite the awareness of the potential of these databases, less is known about ACS registries in the Asia-Pacific region, which accounts for nearly half of the global burden of the disease.
The present study aims to describe the number and characteristics of national registries that are managed by member societies of the Asian Pacific Society of Cardiology (APSC). We also provided an analysis of the number of published articles from these registries and insights into the measures that are needed to achieve to improve outcomes from ACS.
Methods
We searched the APSC website to identify its member countries. As of January 2022, there were 22 member societies under the APSC umbrella from 23 countries.8 We subsequently used Google’s advanced search function to identify publications or reports of any national CVD registries of these member countries.
National registries were selected for the purpose of the current review, given that they are likely to be the largest and more representative of the population than regional or local registries. As such, they are less likely to introduce bias than regional or local registries, which can be affected by practice trends and socioeconomic and cultural factors.
In this study, a national registry was defined as a countrywide system for data collection on cardiac outcomes that was actively collecting data at the time of the search. In the event that a member country had several registries, we selected the registry with the largest sample size, since it would likely be the most comprehensive and representative of the care provided.
We subsequently searched PubMed from database inception until 10 February 2022 for articles related to the national registries identified. This was supplemented with a hand search of article references and citations of articles for additional publications, as well as search on Google Scholar.
Attributes of each article, including title, year, authors and total number of patients included in the registry, were extracted. As the number of citations an article receives is an indicator of its impact and contribution to the clinical practice, we searched for the total number of citations of each published article using citationchaser.9 We also determined journal impact factor and quartile using the Scopus Library database.
As the study only summarised data from registries and did not involve human subjects, no ethical approval was sought.
National Gross Domestic Product and Health Expenditure Data
To shed light on how these registries were used to inform clinical care, we categorised their countries using the World Bank income group classification and the United Nations Statistics Division classification for geographical regions. The annual number of publications in these countries was compared to their healthcare expenditure per capita according to World Bank data.10
Statistical Analysis
All data were presented as median and corresponding interquartile range (IQR) or frequencies. To determine the correlation between the registries and output, we included the inception year, annual gross domestic product (GDP) per capita and healthcare expenditure per capita using Pearson’s correlation coefficient. All statistical analyses were performed using Stata 14.0.
Results
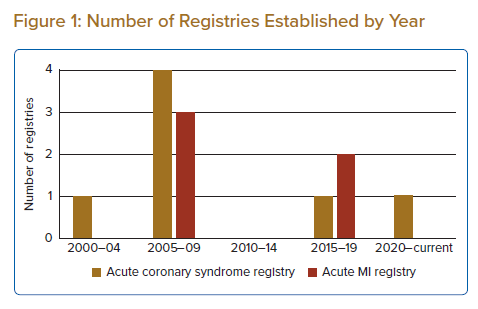
The search found 12 member countries (52.2%) established and maintained active registries, with an almost equal number of ACS (n=7) registries and acute MI (AMI) (n=5) registries. These registries were established from 2002 to 2021, with most established during 2005–09 and 2015–19 (Figure 1).
The registries were primarily established to measure and improve cardiovascular care (Supplementary Table 1). Some also were developed to promote research and guide local development of cardiovascular care and guidelines. Most registries often obtained data about hospital procedures from both public and private settings (Supplementary Table 2).
Bibliographic Analysis
The total number of publications from all 12 databases was 318, a median of 11 (IQR 4.8–13) articles per registry. However, there was a large variation in the number of publications between registries (Supplementary Table 3).
Most articles were from the Korea Acute Myocardial Infarction Registry (KAMIR), which accounted for 304 publications, averaging 16.0 per year. The Thai Acute Coronary Syndrome Registry (TACSR) had the most publications of the ACS registries, with 22 articles, an average of 1.2 per year. In comparison, no publications were generated from several registries, such as the Emirates Cardiac Society (ECS-STEMI) registry and the Cardiac Registry of Pakistan (CROP), according to our searches of PubMed and Google Scholar.
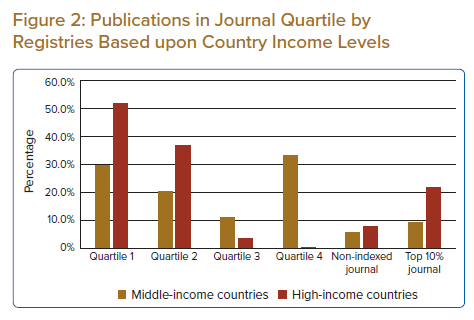
Most articles were published in the top 50% journals in their research areas (83% of total publications), with nearly one in every five (20.1%) published in the top 10% journals in the research field (Figure 2). The five most common journals where these articles were published were the International Journal of Cardiology (n=40; 10.3%), followed by the Journal of Cardiology (n=27; 6.9%), the Korean Circulation Journal (n=24; 6.2%), the American Journal of Cardiology (n=23; 5.9%) and Circulation (n=18; 4.6%). Since 2021, citations of the published articles from these registries ranged from zero to 210, with a median of eight (IQR: 3–18) citations per publication.
Analysis by country income showed that the mean number of publications per registry was much lower from middle-income countries than high-income countries (9.0 versus 83.8). There was a similar disparity in terms of where the articles were published, as high-income countries were able to publish their work from the registry in the top 25% journals in their field more frequently than middle-income countries (51.6% versus 29.6%) (Figure 2).
We subsequently analysed the total number of articles based on countries’ healthcare expenditure per capita, assuming that total healthcare expenditure translated to better healthcare outcomes and resulting publications.
The total healthcare expenditure per article was fairly similar across all middle-income countries’ registries (in a range of US$5–US$52 per publication) except in Iran, where it was much higher at US$121 per publication.
In comparison, this was much higher for high-income countries, which averaged US$380 per publication, except for Korea at US$8.4; however, this was due to the large number of publications as highlighted previously.
There was a poor correlation between number of articles from these registries with GDP per capita, healthcare expenditure per capita and registry inception year.
Discussion
Data comparison has shown that real-world, registry-based data reflect clinical practice.11 As such, information derived from a registry can be used for local guideline development and policy recommendations.
This paper presents an overview of the various registries that have been established by the member countries of the APSC. The number of registries has grown over the past decade, which is not surprising given their many benefits. Indeed, these registries were often developed as a means to identify and monitor unmet medical needs of populations; several are also used to benchmark quality against national targets for use in healthcare policy planning.12,13
The importance of these registries to efforts to improve quality is evident. Registries can provide policymakers and healthcare professionals with information on clinical practice, which forms the cornerstone for all quality improvement initiatives.11,14 For example, they can be used to measure performance and adherence to guidelines as well as monitoring of safety outcomes.
The registries discussed here were often used by the member societies to gauge the performance of healthcare professionals in their country and for quality improvement and benchmarking. For example, the Singapore Myocardial Infarction Registry has been issuing public, annual, risk-adjusted quality-of-care reports, which can be used to inform local hospital policies.
These databases have also facilitated research on large cohorts on ACS patients. Indeed, in our analyses, we noted that nearly all the registries had published the baseline demographics of their cohort and compared their clinical practices and outcomes with those in other settings to see if regional differences in demographics and practice affect outcomes.12,13
While registries have inherent weaknesses, for example voluntary reporting of data, the large datasets provide registry owners with the necessary information to enable their stakeholders to improve outcomes for patients with ACS.
Our study identified many robust national registries, with several member countries having not one but several ACS registries. For example, there were 10 regional ACS registries in Japan, which were subsequently merged into a larger database, the Japan Acute Myocardial Infarction Registry (JAMIR).15 Similarly, we identified two ACS registries in India, the Kerala and CREATE registries.16,17
However, as the aim of our study was to describe and identify ACS registries in the member countries, we selected only the largest registries, on the assumption that this would be the most representative of the countries’ demographics. As such, our search may have omitted some registries because they did not have national coverage or if they had not been developed by APSC members. To mitigate and clarity this, we contacted the members of APSC to ensure we did not miss any relevant information.
Results of our study showed that the number of registries has been increasing and it is likely they will continue to proliferate over the next decade.
Given the considerable resources needed to establish and manage a registry, it is important that researchers and research organisations pay careful consideration to ensure that any new registry will take a synergistic approach.
For example, funders and policymakers should consider developing infrastructure that will generate the most high-quality data in terms of ensuring high patient enrolment and retention, with high reliability, with data validation incorporated throughout the process. This will ensure that any data generated could be used to inform health policies, as well as to facilitate future areas for research and monitoring the uptake of new treatments.
Among all the registries of the member countries, one registry is particularly worthy of mention, namely KAMIR.18 Our analysis noted that KAMIR, set up in 2005 in South Korea, was the most successful registry, with a total of 304 articles published since its inception. Analysis of baseline demographics and clinical characteristics of participants in the KAMIR registry revealed baseline differences in the cohort characteristics compared to registries from North America and Europe. Given these differences, researchers have used the information to improve their practice (e.g. transfer protocols for patients who arrive at STEMI referral centres), which has led to improved outcomes of percutaneous coronary interventions and, ultimately, patient mortality.19
Our analysis also found a poor correlation between some of the measures of national economic output and healthcare expenditure. This finding was because KAMIR had published multiple articles and this had skewed the data. Exclusion of this registry data from the analysis showed that the average papers per registry would be very similar between middle- and high-income countries, at 9.0 versus 7.8 publications per registry, respectively. Exclusion of KAMIR would also result in a small change in the correlation, with a positive correlation between the total number of papers with healthcare expenditure in high income countries.
Nearly two-thirds (n=264; 67%) of these articles were published in cardiology-specific journals, such as the American Heart Journal, the American Journal of Cardiology, the Journal of Cardiology and Circulation among others. This result is not surprising, given that these were cardiology-specific registries so would be of interest to the readers of these journals rather than those of general medicine publications. Only one article generated by these registries was published in the Journal of the American Medical Association, which was the most highly cited article among all these papers.20
Limitations
Our study has several limitations. First, we performed searches using only PubMed and Google Scholar and used terms in English. It is possible that we may have missed some databases that could have been listed in the native language; Thai, Korean and even Chinese databases were not indexed in the databases mentioned above.
Second, we did not assess the quality of the registries in this study. As several studies have noted, registry quality varies, which may partly explain the differences in the total publications generated from each registry.21,22 As the value of a registry in achieving its aims is determined by the accuracy and completeness of data, we used the number of total citations as a surrogate for registry quality.
Third, we acknowledge that there may be publication drafts from these 12 registries that have been accepted by peer-reviewed journals but are not accounted for in our study as they would not have been found on our search databases.
Finally, as we included national registries in this study, large regional registries or international registries in which some member countries of the APSC could have participated would not have been included.
As with many other bibliometric analyses, the study analysis favours older published articles since these are likely to have generated more citations than newer articles. Our analysis also did not take into consideration the inherent issue associated with self-citations.
Recommendations
Developing and maintaining a registry is a complex task which is a major barrier to their widespread use in many countries. Given this arduous task, it is imperative that a repository of registries, detailing the aims and data sets collected, is available to researchers to avoid data duplication in yet to be developed future registries.
In this regard, the APSC could take the leading role in coordinating the effort to provide expertise in facilitating the establishment of an international cross-border CVD registry for its member countries. Through this, it is hoped that data collected can be harmonised, which can help facilitate transnational comparison of the quality of cardiovascular care in the region.
Conclusion
This article provides an insight into the national ACS and AMI registries established by APSC members. There are differences in terms of outputs and quality of articles stemming from them, which may reflect the differences in the quality of these registries and how complete their data are.
Nevertheless, these national registries provide vital contributions to the improvement of treatment outcomes of patients with ACS and AMI and would be instrumental to establishing national or even regional Asian guidelines for ACS and AMI.
Click here to view Supplementary Material.
Clinical Perspective
- The proliferation of therapies and clinical guidelines in cardiovascular disease suggests that there is a gap in translating clinical evidence to widespread clinical practice. In response, several Asian Pacific Society of Cardiology member countries have developed acute coronary syndrome and MI registries.
- The registries are used for various purposes, the most common being to improve the quality of care, monitor patient safety and drive clinical research.
- There were differences in terms of outputs and quality of publications stemming from these registries, which may reflect the differences in how they are organised and run.